Vitamin D3 Oral Solution (liquid drops or oil solutions) are a convenient, accurately dosed way to deliver cholecalciferol — especially for infants, people who have trouble swallowing pills, or anyone needing fast absorption. They’re often preferred for infant supplementation (400 IU/day recommended), and some liquid formulations show equal or faster absorption than tablets or capsules. However, dosing must be accurate and monitored because excess vitamin D can cause hypercalcemia and other serious problems.
Table of Contents
Why this guide matters
You asked for an in-depth, actionable article on vitamin D3 oral solution: what it is, when to use it, how to dose it (infants through adults), how liquid formulations compare to tablets and capsules, safety signals (upper limits and toxicity), and how to pick a reputable product. I also include product / affiliate ideas, an internal linking plan for VigorBlog, and image suggestions so the page is ready to publish.
What is a vitamin D3 oral solution?
Vitamin D3 (cholecalciferol) is the animal/skin-derived form of vitamin D. When sold as an oral solution it’s typically formulated as a concentrated liquid (oil-based or micellar/nanoemulsion) delivered with a calibrated dropper or a measured spoon. These liquid formats are commonly labeled as “drops” or “oral solution” and often give strength in IU per drop (for example, 400 IU/drop or 10 mcg/drop) or IU per mL. Commercial infant formulas and adult maintenance products exist across many strengths.
Top reasons people choose a liquid
- Easy dosing for infants and kids — droppers make it simple to give precise small doses (e.g., 400 IU/day for infants).
- Better for people who can’t swallow pills — older adults, people with dysphagia, or anyone avoiding tablets.
- Potentially faster / higher early absorption — some studies show oral solutions (nano-/micellar formulations) can produce higher early blood levels (Cmax/AUC) versus conventional tablets or softgels. This can be helpful for rapid repletion regimens.
- Flexible dosing — dropper bottles allow splitting or combining doses as the prescriber recommends.
Key clinical dosing guidance
Infants (0–12 months): 400 IU (10 µg) daily is recommended for breastfed or partially breastfed infants (start soon after birth) — the AAP and major pediatric guidance support this. Formula-fed infants receiving ≥32 oz (≈1 L) of fortified formula/day may not need extra supplements.
Children (1–18 years): usual recommended intake ~600 IU/day for most healthy children; higher doses (e.g., 1,000–2,000 IU) may be used under medical supervision for deficiency or at-risk groups.
Adults (19–70 years): RDA 600 IU/day (some individuals need more); tolerable upper intake level (UL) is typically set at 4,000 IU/day for most adults — higher therapeutic regimens are sometimes used briefly under medical supervision.
Practical note: Many oral solution products label the IU per drop or per 0.5 mL — always check the container so you deliver the correct quantity (and never assume every “1 drop” equals the same IU across brands). If your infant product says 400 IU per 0.5 mL, one must follow that exact dropper volume.
Liquid vs tablet/capsule: which is better?
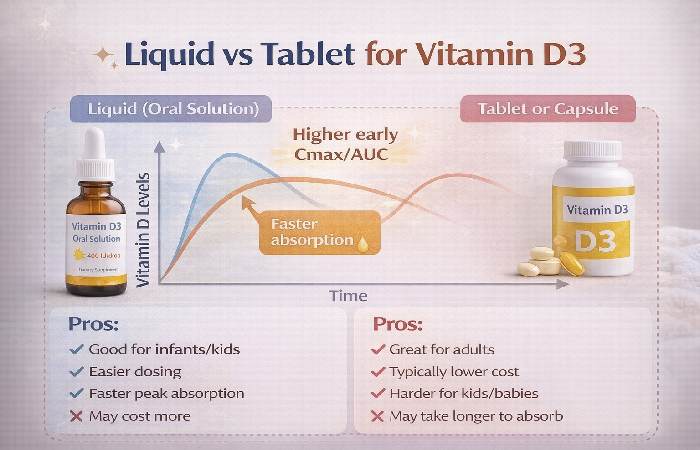
Short answer: both work — but liquid solutions have advantages in dosing and early absorption for certain patients.
- Evidence: Multiple pharmacokinetic and clinical studies show some oral solutions (including nanoemulsion/micellar formulas) produce higher early Cmax and AUC values than conventional tablets or capsules and may replete 25(OH)D more quickly in some settings. However, overall outcomes (bone health, symptoms) depend on dose and duration rather than on delivery form alone.
- When to pick liquid: infants, people who need small or fractional dosing, patients who are malnourished or have swallowing problems, or when the clinician wants fast repletion.
- When tablets are fine: routine long-term maintenance for adults who can swallow pills and want a stable, typically lower-cost option.
Safety & toxicity — what to watch for
- Upper limit (UL): Population UL is commonly referenced at 4,000 IU/day for adults; ULs for infants/children are lower (see table below). Staying within these ULs, unless supervised by a clinician, reduces the risk of toxicity.
- Toxicity (hypervitaminosis D): caused almost exclusively by excess supplementation. Symptoms include nausea, vomiting, weakness, polyuria, polydipsia, confusion, and — most importantly — hypercalcemia (high blood calcium), which can damage the kidneys and the heart. Recent regulatory recalls show why careful dosing and quality control matter — contaminated or mis-labeled products have occasionally produced dangerously high doses.
Quick reference: RDA & Upper Limits
| Age group | Typical recommended intake | Tolerable upper intake level (UL) |
| Infants 0–6 months | 400 IU/day (Adequate Intake) | 1,000 IU/day |
| Infants 7–12 months | 400 IU/day | 1,500 IU/day |
| Children 1–3 yrs | 600 IU/day | 2,500 IU/day |
| Children 4–8 yrs | 600 IU/day | 3,000 IU/day |
| Adolescents 9–18 yrs | 600 IU/day | 4,000 IU/day |
| Adults (19–70+) | 600 IU/day (varies) | 4,000 IU/day. |
How to choose a safe, effective vitamin D3 oral solution
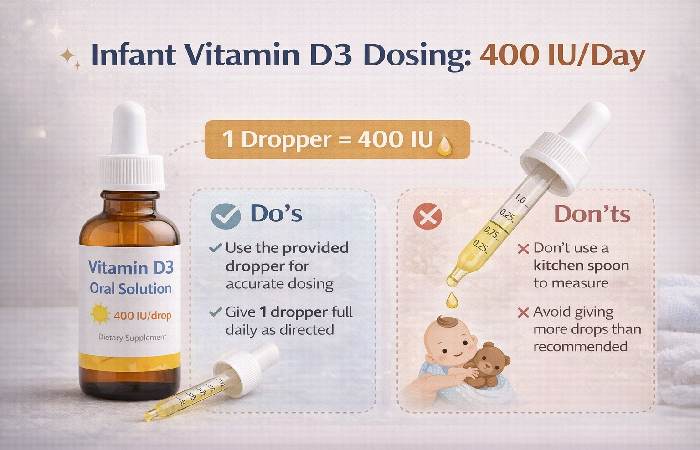
- Check the IU per dose — infant products often specify 400 IU per 0.5 mL or 10 mcg/drop. Confirm how many drops equals the labeled dose.
- Prefer cholecalciferol (D3) for most people — it raises and maintains 25(OH)D levels more effectively than vitamin D2 in numerous studies.
- Third-party testing: look for USP, NSF, or other independent testing statements or COA (certificate of analysis) availability.
- Carrier/base matters — many infant drops use oil bases (sunflower/olive oil) for absorption; newer micellar or nano-emulsions are engineered to improve bioavailability.
- Avoid mega-doses without a lab test — do not self-prescribe high daily doses (e.g., >4,000 IU/day long term) without monitoring 25(OH)D and calcium.
Practical dosing examples
- Product label: “400 IU per 0.5 mL” — use the supplied dropper to measure 0.5 mL once daily for infants.
- Product label: “10 IU per drop” (less common) — compute required drops carefully.
- If you switch brands, reconfirm the IU per drop — droppers vary and so do concentrations.
Clinical use cases & protocols
- Routine infant prophylaxis: 400 IU/day liquid drops for breastfed infants (start soon after birth).
- Deficiency treatment: clinicians may use weekly higher doses (e.g., 50,000 IU weekly for several weeks) or daily repletion regimens — oral solutions have been used in such protocols; monitor labs.
- Maintenance in adults: 600–2000 IU/day depending on baseline 25(OH)D, exposure, and comorbidities. Stay under UL without supervision.
Product & affiliate ideas
- Infant vitamin D3 oral drops (400 IU/dropper bottle) — high buyer intent. (Example product pages exist from various manufacturers.
- Adult micellar / nano-emulsion vitamin D3 — marketed for better absorption.
- Measuring droppers / dosing syringes (for accurate dosing)
- Home 25(OH)D testing kits (affiliate option to encourage safe monitoring)
- Bundle idea: infant vitamin D3 + vitamin D education lead magnet (email list sign-up).
Common FAQs
Q: Is vitamin D3 oral solution the same as vitamin D drops?
Yes — “oral solution” and “drops” are often used interchangeably; strengths and droppers vary, so check the label.
Q: Are liquid D3s safe for newborns?
Yes, when dosed correctly. The American Academy of Pediatrics recommends 400 IU daily for breastfed infants.
Q: Can I use an adult oral solution on my baby?
No — adult formulations often have much higher concentrations per mL. NEVER use an adult product for infants unless a clinician prescribes and demonstrates dosing.
Q: Can you get vitamin D from sun exposure instead of drops?
Sun produces vitamin D, but infants are generally not recommended for direct sun exposure; supplementation is a safe way to ensure 400 IU/day in breastfed infants.
Final Thoughts
Vitamin D3 oral solutions offer a practical, flexible way to support healthy vitamin D levels — especially for infants, older adults, and anyone who prefers liquid supplements over tablets. Their easy dosing, quick absorption potential, and suitability for people who struggle with swallowing pills make them a popular choice in both preventive care and deficiency management. However, accuracy matters: always follow the labeled dose or your healthcare provider’s guidance to avoid under- or over-supplementation.
Quality and consistency should also guide your decision. Choose reputable brands, check the IU strength carefully, and look for third-party testing or certifications when possible. Pair supplementation with healthy habits like balanced nutrition, sensible sun exposure, and regular health checkups to maintain optimal vitamin D status.
Ultimately, a vitamin D3 oral solution can be a safe and effective supplement when used responsibly, helping support bone health, immune function, and overall well-being.